 |
Case Report
Congenital laryngocele: An uncommon cause of neonatal respiratory distress
1 Otorhinolaryngology Unit, Department of Surgery, Ben Carson College of Health and Medical Sciences, Babcock University, Ilishan Remo, Nigeria
2 Department of Surgery, Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria
3 Department of Surgery, College of Medicine, University of Lagos, Idi-Araba, Lagos, Nigeria
Address correspondence to:
Moses Ayodele Akinola
Otorhinolaryngology Unit, Department of Surgery, Ben Carson College of Health and Medical Sciences, Babcock University, Ilishan Remo,
Nigeria
Message to Corresponding Author
Article ID: 100007Z18OP2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Olusoga-Peters O, Akinola MA, Adumah CC, Bamigboye BA, Alao OJ. Congenital laryngocele: An uncommon cause of neonatal respiratory distress. J Case Rep Images Otolaryngol 2022;3(2):7–11.ABSTRACT
Introduction: Congenital laryngocele is a rare phenomenon as only a few cases have been reported in literature. It is a pathologic occurrence originating in the saccule of the laryngeal ventricle. In many cases, patients with congenital laryngoceles present with respiratory distress due to the narrow airway of the neonate necessitating urgent surgical management.
Case Report: We present a 29-day-old male neonate referred by the pediatrics team of our facility on account of respiratory distress, regurgitation of feeds, and a left-sided neck mass since birth. Evaluation of the patient included neck ultrasound, direct laryngoscopy of the larynx, and computed tomography (CT) scan of the neck. The imaging revealed a cystic mass containing air, compressing the airway. Surgical intervention via the external cervical approach was used to excise the mass, following an intra-operative tracheostomy. The child did well during the post-operative period and on follow-up, no sign of recurrence was observed.
Conclusion: Congenital laryngocele might lead to obstruction of airway necessitating tracheostomy in neonate. We report the first case of congenital laryngocele in our environment and discuss the management.
Keywords: Airway obstruction, Congenital, Laryngocele, Tracheostomy
Introduction
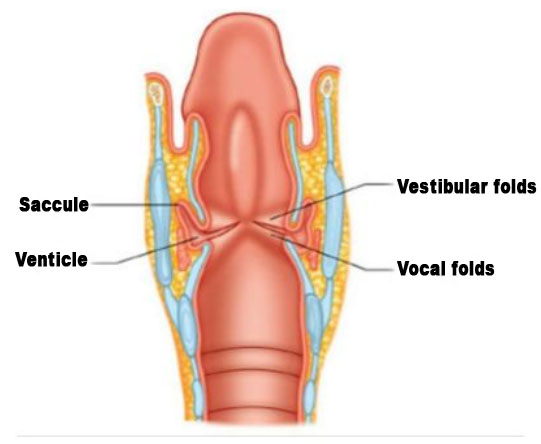
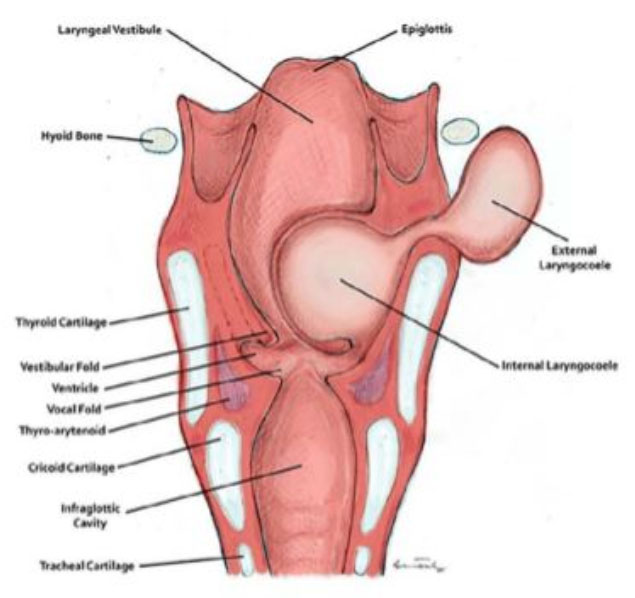
Laryngocele is an abnormal cystic dilatation of laryngeal saccule of the laryngeal ventricle (Figure 1) and communicate with the laryngeal lumen. Laryngomucocoele and laryngopyocoele are seen when the sac is filled with mucous or pus respectively [1],[2]. They are mostly unilateral and benign [3]. It is found to be unilateral in 85% of cases and bilateral in 15% of cases [4]. It is a rather rare condition of 1 in 2.5 million [5]. The peak incidence is between ages 50 years and 60 years and more common in male than female [6]. It may be congenital or acquired depending on the etiology. Laryngocele has been recently classified into two types, namely internal and mixed (combined, Figure 2) with respect to the relationship of the laryngocele to the thyrohyoid membrane [7]. The most common type of laryngocele is the combined type. The risk factors include congenital factors, increased intra-laryngeal pressure, and mechanical obstruction [4]. Congenital laryngocele, though a benign lesion, may lead to significant upper airway obstruction necessitating emergency intervention [8]. Management of laryngocele is usually based on the type and advancement of the condition.
We report a case of respiratory distress in a 29-day-old male on account of congenital laryngocele and discuss the clinical presentation, diagnosis, and treatment.
Case Report
Our patient is a 29-day-old male neonate who was referred by the pediatrics team of our facility on account of respiratory distress and regurgitation of feeds and a left-sided neck mass since birth which has been increasing in size. He was a normal appearing 2500 g, full-term baby with no significant prenatal medical history and he had APGAR score of 8 at 1 and 9 at 5.
On examination, he was in obvious respiratory distress with respiratory rate of 50 cycles per minute and had 94% oxygen saturation on intranasal oxygen. There was a soft, cystic mass on the left side of neck about 2 cm by 2 cm in size, conducting vibration on crying and coughing, manually reducible and covered with normal skin (Figure 3). The mass was aspirated, revealing mostly air and a thick yellowish mucoid effluent. No history or examination suggestive of other congenital malformation.
A computed tomography (CT) scan described a 25 mm by 22 mm well circumscribed thin-walled air-filled mass on the neck extending to the airway with narrowing of the laryngeal air column. The 3D image is shown in Figure 4.
Pre-operative workup was done for the patient and consent was taken for excision of laryngocele ± tracheostomy in case of difficult intubation. Prior to surgical excision of the mass, there was a need to perform a tracheostomy as the baby could not be intubated (Figure 3). Direct laryngoscopy augmented with 2.7 0° endoscope was done under general anesthesia before the excision of the neck mass which showed a left-sided supraglottic mass covered with normal mucosa extending into the airway with significant narrowing of the larynx (Figure 5). Excision of the laryngocele was performed via an external cervical approach (Figure 6). The post-operative period was uneventful with antibiotic [intravenous (iv) ceftriaxone)], analgesic, and steroid. He was decannulated three days post-op. Following decannulation, no pre-operative symptoms (stridor and respiratory distress) were observed. The stoma and left lateral neck wounds were well apposed. Histologic report confirmed diagnosis of congenital laryngocele. A repeat endoscopy was not carried out post-surgery due to lack of pediatric flexible laryngoscope in our center, but the patient has been stable with no sign of recurrence of preoperative complaints and neck mass. At six months post-surgery, the baby was noticed to be healthy with no feature suggestive of recurrence (Figure 7).





Discussion
Laryngocele is rare and was first reported as air containing tumors in 1829. However, the first laryngeal cyst in a newborn was published in 1876 [9]. Laryngocele is an air-filled mass arising from herniation of the laryngeal saccule which is a blind-ended structure that opens into the laryngeal ventricle [5]. The laryngeal ventricle is a fusiform fossa situated between the false and true vocal folds (Figure 1).
The laryngocele in early childhood is congenital and acquired in adults. Congenital laryngocele developed as a result of congenital dilatation of the saccule as seen in our patient. The acquired laryngocele developed because of increased laryngeal pressure from straining activities like lifting of heavy object and blowing of wind instrument [7].
Laryngocele has been divided into two types depending on its relationship with the thyrohyoid membrane which can be internal or mixed. In the internal type of laryngocele the sac is within the thyroid cartilage while in the mixed type the sac protrudes through the thyroid membrane and seen as a smooth compressible neck mass. Laryngocele may be asymptomatic; however, the main symptoms are usually cough, hoarseness, stridor, dyspnea, and visible neck mass. The mixed type of laryngocele usually presents with combined symptoms of external and internal types as seen in our patient who presented with an external lateral neck mass and features of airway obstruction respectively [6],[10].
It is usually difficult to diagnose or envisage airway obstruction prenatally but; however, this becomes visible as soon as the child is born as seen in our patient [8].
Depending on the size and type of laryngocele, the clinical presentation varies. Nonetheless, in neonates, small laryngoceles may cause severe respiratory distress due to obstruction of the narrow airway off the neonate as seen in our patient, hence a possible need for intubation or tracheostomy [11],[12].
Congenital laryngocele has been diagnosed with combination of the presenting symptoms, physical examination of the neck, and findings on laryngoscopy. These radiological images, such as CT and MRI, have been used to support the diagnosis [8],[13].
Concerning diagnostic imaging for laryngoceles, CT scans have been shown to be the most accurate radiologic investigation in demonstrating location of the laryngocele and the spatial relationship between the laryngocele and surrounding structures and ruling out other related laryngeal pathologies such as cancer [13]. Magnetic resonance imaging has also been shown to be helpful in diagnosing laryngocele [14].
Congenital laryngocele commonly present with airway compromise and the need for creating alternative airway is important in neonates as seen in our patient who had tracheostomy prior to excision of the laryngocele due to difficult intubation [8].
Laryngocele can be approached via an external or endoscopic resection. External cervical approach is preferred in mixed type while endoscopic resection is preferable in internal laryngocele [9],[10]. External approach was used in our patient due to the mixed nature of the laryngocele. Other techniques of resection such as endolaryngeal microlaryngoscopy, carbon dioxide laser excision, and transoral robotic surgery have been suggested in other studies [12],[15]. As also described in this study and any others, there is usually a need to prevent post-operative edema by administration of steroid. Six months follow-up revealed that our patient is doing well following the excision of the mass via the external approach with no sign of recurrence.
Conclusion
Congenital laryngocele is one of the rare etiologies of upper airway obstruction in neonate. In view of the narrow airway of the neonate, urgent intubation or tracheotomy may be required to stabilize the patient before definitive surgery. External approach is still favored in the management of combined type of laryngocele to ensure complete resection.
REFERENCES
1.
Weissler MC, Fred MP, Kelly JH. Laryngopyocele as a cause of airway obstruction. Laryngoscope 1985;95(11):1348–51. [CrossRef]
[Pubmed]

2.
Kapoo NN, Amitabha R. Textbook of Laryngology. India: Jaypee Brother Medical; 2018. p. 11.
3.
Detsouli M, Chelly H, Essaadi M, Mokrim B, Touhami M, Benchekroun Y. Laryngocele as an etiology of respiratory distress. [Article in French]. Ann Otolaryngol Chir Cervicofac 1994;111(8):476–8.
[Pubmed]
4.
Mobashir MK, Basha WM, Mohamed AE, Hassaan M, Anany AM. Laryngocoele: Concepts of diagnosis and management. Ear Nose Throat J 2017;96(3):133–8. [CrossRef]
[Pubmed]
5.
Stell PM, Maran GD. Laryngocoele. J Laryngol Otol 1975;89(9):915–24. [CrossRef]
[Pubmed]
6.
Pennings RJ, van den Hoogen FJ, Marres HA. Giant laryngoceles: A cause of upper airway obstruction. Eur Arch Otorhinolaryngol 2001;258(3):137–40. [CrossRef]
[Pubmed]
7.
James DL, Garry S, Corbett M, Lang J. Mixed infected laryngocoele presenting as airway obstruction: A case report. J Surg Case Rep 2021;2021(2):rjaa615. [CrossRef]
[Pubmed]
8.
Taskinlar H, Vayisoglu Y, Avlan D, Polat D, Nayci A. Congenital laryngomucocele: A rare cause of airway obstruction in newborn. J Craniofacial Surg 2015;26(3):e238–40. [CrossRef]
[Pubmed]
9.
Borkó R, Szûcs S. Congenital laryngeal cysts. [Article in German]. HNO 2000;48(11):843–5. [CrossRef]
[Pubmed]
10.
Zelenik K, Stanikova L, Smatanova K, Cerny M, Kominek P. Treatment of laryngoceles: What is the progress over the last two decade? Biomed Res Int 2014;2014:819453. [CrossRef]
[Pubmed]
11.
Ambrus A, Sztanó B, Szabó M, Vasas B, Sziller I, Rovo L. An unusual cause of infant’s stridor – congenital laryngocele. J Otolaryngol Head Neck Surg 2020;49(1):34. [CrossRef]
[Pubmed]
12.
Ahmed H, Ndiaye C, Barry MW, et al. A rare cause of upper airway obstruction in a child. Case Rep Otolaryngol 2017;2017:2017265. [CrossRef]
[Pubmed]
13.
U?uz MZ, Onal K, Karagöz S, Gökçe AH, Firat U. Coexistence of laryngeal cancer and laryngocele: A radiologic and pathologic evaluation. [Article in Turkish]. Kulak Burun Bogaz Ihtis Derg 2002;9(1):46–52.
[Pubmed]
14.
Robinson ED, Wekhe C. The role of magnetic resonance imaging in the diagnosis of bilateral laryngocele. Muller J Med Sci Res 2020;11(2):102–5. [CrossRef]
15.
Y?lmaz S, Y?ld?zba? S, Yaman H, Güçlü E, Öztürk Ö. Stridor in a newborn caused by a congenital laryngocele and bifid epiglottis: A case report and review of literature. International Journal of Pediatric Otorhinolaryngology Extra 2010;5(1):28–31. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Oluwapelumi Olusoga-Peters - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Moses Ayodele Akinola - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Collins Chijioke Adumah - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Babatunde Akinola Bamigboye - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Oluwaseyi Joy Alao - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Oluwapelumi Olusoga-Peters et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



