 |
Clinical Image
Non-recurrent laryngeal nerve: A rare anatomical variant
1 Department of Clinical Surgical Sciences, University of West Indies, Eric Williams Medical Sciences Complex, Champs Fleur, Trinidad and Tobago
Address correspondence to:
Nicholas Figaro
Department of Surgery, Eric Williams Medical Sciences Complex, Uriah Butler Highway, Champ Fleurs,
Trinidad and Tobago
Message to Corresponding Author
Article ID: 100013Z18NF2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Figaro N, Badall A, Arozarena R, Juman S. Nonrecurrent laryngeal nerve: A rare anatomical variant. J Case Rep Images Otolaryngol 2024;5(2):4–6.ABSTRACT
No Abstract
Keywords: Ear, nose, and throat, Fine needle aspiration, Non-recurrent laryngeal nerve, Recurrent laryngeal nerve
Case Report
A 60-year-old female with a history of well-controlled asthma presented to the ear, nose, and throat (ENT) outpatient clinic with a one-year history of left anterior neck swelling. Initial ultrasonography revealed a solitary left lobe TIRADS 5 nodule without cervical lymphadenopathy. Physical examination identified a 3 cm × 2 cm firm mass in the left thyroid lobe, with normal vocal cord function observed on flexible laryngoscopy. Fine needle aspiration (FNA) of the nodule indicated features consistent with papillary thyroid carcinoma. Computed tomography (CT) of the neck and chest confirmed the presence of the left thyroid nodule, again without cervical lymphadenopathy or other abnormalities.
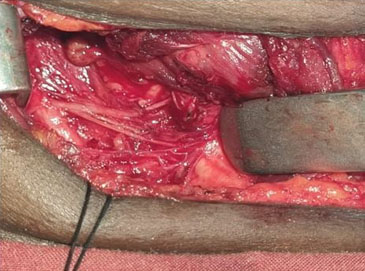
A total thyroidectomy was planned. Intraoperatively, the left lobe was found to be largely replaced by a 3 cm × 3 cm hard mass. Despite successful identification of the left recurrent laryngeal nerve (RLN) in its recurrent position, the nerve was inadvertently injured during the challenging dissection process. Given this consideration, meticulous dissection of the right lobe was performed; however, the RLN was not found in its typical anatomical location. Continued dissection eventually revealed a nerve perpendicularly entering the cricothyroid joint, identified as a branch of the vagus nerve (Figure 1).
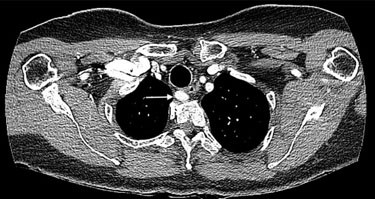
Immediately postoperatively, the patient presented with hoarseness but no respiratory distress. On postoperative day one, flexible laryngoscopy revealed an immobile left vocal cord. A subsequent review of preoperative CT images, which initially overlooked this detail, identified an aberrant retroesophageal right subclavian artery (Figure 2).
Pathological examination of the surgical specimen confirmed multifocal classical type papillary carcinoma without extra-thyroidal extension or vascular invasion, staged as pT2N0M0. Postoperatively, the patient underwent I-131 therapy.
Discussion
The non-recurrent laryngeal nerve (NRLN), a rare anatomical variant of the recurrent laryngeal nerve (RLN), typically arises from partial developmental anomalies of the pharyngeal apparatus during embryogenesis [1]. In the general population, the prevalence of right-sided NRLN ranges from 0.3% to 1.6% [2]. Conversely, the left-sided NRLN is exceedingly rare, with a prevalence of only 0.04%, as its occurrence necessitates the presence of situs inversus or a right-sided aortic arch [1].
The embryological basis for the right-sided NRLN is attributed to a vascular anomaly known as arteria lusoria [1]. In this condition, the fourth aortic arch on the right side involutes rather than persisting to form the subclavian artery. Consequently, the right recurrent laryngeal nerve (RLN) is not drawn inferiorly during the descent of the heart and the elongation of the neck in embryogenesis. As a result, the RLN emerges higher in the neck rather than at its root, proceeding directly to the larynx as the NRLN. In this scenario, the right subclavian artery originates from the left side of the aortic arch and traverses posterior to the esophagus [1],[3]. Left NRLNs are exceptionally rare, as their occurrence necessitates the presence of a combination of uncommon vascular anomalies. Specifically, three conditions must be met for the nerve to assume this position on the left side: the presence of a right-sided aortic arch, an aberrant right subclavian artery, and the absence of the ductus arteriosus or its remnants [4]. From an embryological perspective, the recurrent laryngeal nerve is intricately linked to the development of the fourth, fifth, and sixth branchial arches on both sides. During embryogenesis, the fifth and sixth arches on the right side are typically reabsorbed, leaving the right recurrent laryngeal nerve to loop beneath a fourth arch structure, specifically the right subclavian artery. Conversely, on the left side, the nerve loops around both the fourth arch, which becomes the adult aortic arch, and the sixth arch, which gives rise to the ductus arteriosus, as the fifth arch generally regresses. The formation of a left NRLN requires the further regression of both the fourth and sixth primitive aortic arches. Consequently, a right-sided aorta arises because the right fourth arch is solely responsible for its development [4].
Approximately 5% of patients with this vascular malformation will experience dysphagia, known as dysphagia lusoria, due to compression of the esophagus by the retro-esophageal artery [3],[5]. However, the patient in our case report did not report any symptoms of dysphagia.
Three types of NRLNs have been delineated. In type 1, the nerve courses alongside the superior vascular pedicle of the thyroid gland. In type 2a, the nerve runs superior to the trunk of the inferior thyroid artery. In type 2b, the nerve traverses either below the trunk or between the branches of the inferior thyroid artery [2],[6].
The NRLN is more susceptible to surgical injury because of its unusual anatomical position. These injuries may lead to long-term postoperative complications, such as vocal cord paralysis [7] .
Recent research has demonstrated that patients with a preoperatively undiagnosed NRLN are at an approximately six-fold increased risk of intraoperative nerve damage [6]. Additionally, these studies have shown that the majority of NRLN injuries occurred in patients whose nerves originated above the laryngotracheal junction and followed the course of the superior thyroid artery (type 1) [7] .
The presence of a NRLN can be predicted by identifying an arteria lusoria and the absence of the brachiocephalic artery on a preoperative CT scan [8]. Additionally, preoperative ultrasonography can reliably predict the presence of an NRLN by detecting arterial anomalies that are consistently associated with this nerve variation. Ultrasonography, being a simple and highly reliable method, plays a crucial role in the preoperative assessment of vascular anomalies linked to NRLN, thereby aiding in optimal surgical decision-making to minimize the risk of nerve damage during thyroidectomy [9].
Additionally, the RLN and its anatomical variant, the NRLN, can be effectively identified through the use of intraoperative nerve monitoring (IONM). However, the availability of IONM is not widespread, particularly in resource-limited centers, and its routine use may be deemed financially impractical in some surgical environments [7]. In our case, we did not utilize IONM due to its unavailability in our facility.
Thyroid surgeons typically adhere to a surgical principle aimed at mitigating significant nerve injury. During thyroidectomy, it is recommended to perform systematic and meticulous dissection guided by typical anatomical landmarks, while consistently considering the potential for anatomical variations [7]. It is generally advised that no transverse band, except for the middle thyroid vein, should be severed unless the RLN is first identified and preserved [3],[5]. By employing this operative technique, we were able to identify a right NRLN in this case.
Conclusion
The incidence of NRLN is very rare, but its presence significantly increases the risk of damage during thyroidectomy. Preoperative imaging diagnosis of arteria lusoria and dysphagia lusoria may suggest the presence of a NRLN. Although auxiliary methods such as intraoperative neuro-monitoring can assist in identifying the RLN during surgery, systematic and meticulous dissection based on standard anatomical landmarks, coupled with an awareness of the potential for NRLN, remains the gold standard technique to minimize morbidity.
REFERENCES
1.
Henry BM, Sanna S, Graves MJ, et al. The non-recurrent laryngeal nerve: A meta-analysis and clinical considerations. Peer J 2017;5:e3012. [CrossRef]
[Pubmed]

2.
Guerreir S, Lamas M, Candeias H, Eusébio R, Rocha V. The non-recurrent laryngeal nerve: An anatomical “trap.” Rev Port Endocrinol Diabetes Metab 2014;9(1):84–7. [CrossRef]
3.
Forde R, Williams EW. The non-recurrent laryngeal nerve—A rare phenomenon which requires vigilance. West Indian Med J 2015;64(3):303–4. [CrossRef]
[Pubmed]
4.
Ahumada NG, Hojaij FC, Cunico C, Akahane HGK, Leitão CA, Matias JEF. Left nonrecurrent laryngeal nerve: A very unusual finding during thyroid surgery. Case Rep Surg 2022;2022:4632501. [CrossRef]
[Pubmed]
5.
Morais M, Capela-Costa J, Matos-Lima L, Costa-Maia J. Nonrecurrent laryngeal nerve and associated anatomical variations: The art of prediction. Eur Thyroid J 2015;4(4):234–8. [CrossRef]
[Pubmed]
6.
Raj S, Deo RP, Mohiyuddin A, Merchant S, Ramachandra M. Nonrecurrent laryngeal nerve: An Indian documentation. Int J Head and Neck Surg 2012;3(1):28–9. [CrossRef]
7.
Tesso BA, Tola GG, Abadura MA. A case report of the rare non recurrent laryngeal nerve in a resource limited setting: The first Ethiopian documentation. Int J Surg Case Rep 2023;110:108751. [CrossRef]
[Pubmed]
8.
Watanabe A, Kawabori S, Osanai H, Taniguchi M, Hosokawa M. Preoperative computed tomography diagnosis of non-recurrent inferior laryngeal nerve. Laryngoscope 2001;111(10):1756–9. [CrossRef]
[Pubmed]
9.
Citton M, Viel G, Iacobone M. Neck ultrasonography for detection of non-recurrent laryngeal nerve. Gland Surg 2016;5(6):583–90. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Nicholas Figaro - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asa Badall - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rodolfo Arozarena - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Solaiman Juman - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Nicholas Figaro et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



