 |
Case Report
Functioning middle ear neuroendocrine tumor: A rare case of systemic activity
1 Division of Otorhinolaryngology, University of Florida, Jacksonville, USA
Address correspondence to:
Nirmal Thapa
MD, 653-1 W. 8th Street, 4th Floor, LRC, Jacksonville, FL 32209,
USA
Message to Corresponding Author
Article ID: 100015Z18NM2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Minaya NJ, Thapa N. Functioning middle ear neuroendocrine tumor: A rare case of systemic activity. J Case Rep Images Otolaryngol 2025;6(2):1–4.ABSTRACT
Introduction: Middle ear neuroendocrine tumors (MeNETs) are rare neoplasms with dual epithelial and neuroendocrine differentiation. They typically present as indolent lesions with nonspecific symptoms, making diagnosis challenging.
Case Report: We present a case of a functioning MeNET in a 59-year-old male with left-sided hearing loss, ipsilateral postauricular and occipital pain, and systemic symptoms suggestive of neuroendocrine activity. Surgical excision and histopathology confirmed a grade 1 neuroendocrine tumor.
Conclusion: This case represents the first reported instance of a functioning MeNET, broadening the understanding of this tumor’s potential systemic activity. It highlights the importance of thorough clinical evaluation, surgical management, and long-term surveillance, as well as the need for further research into the pathophysiology of MeNETs.
Keywords: Comertise carcinoid tumor, Functioning MeNET, Middle ear adenoma, Neuroendocrine tumor
Introduction
Middle ear neuroendocrine tumors (MeNETs) are exceptionally rare neoplasms with both epithelial and neuroendocrine differentiation, representing less than 2% of primary tumors in the middle and inner ear [1]. These tumors were first documented in 1976 by Hyams and Michaels [2] and were further characterized in 1980 by Murphy et al. [3]. Since then, over 140 cases have been reported in the English literature, with various terms used to describe them, including middle ear adenoma, middle ear adenomatous neuroendocrine tumor, and middle ear carcinoid tumor [4],[5].
Middle ear neuroendocrine tumors generally exhibit indolent biological behavior, manifesting as benign-appearing lesions with slow local growth. Due to their nonspecific clinical presentation and radiological features, diagnosis can be challenging. The mainstay of treatment is complete surgical excision. We report a case of a functioning MeNET and a review of the literature.
Case Report
A 59-year-old male presented with left-sided “muffled” hearing of unspecified duration, accompanied by ipsilateral postauricular and occipital pain. Microscopic examination of the left ear revealed a dull, bulging pars flaccida, and pars tensa of the tympanic membrane, with absence of the light reflex. The right ear examination was unremarkable.
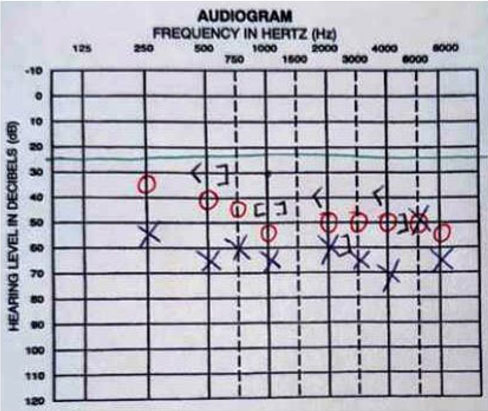
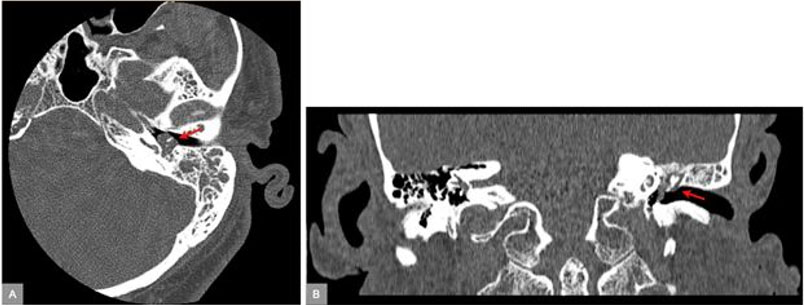
Pure-tone audiometry demonstrated moderate to severe mixed hearing loss in the left ear and mild to moderate sensorineural hearing loss (SNHL) in the right ear across frequencies from 250 to 8000 Hz (Figure 1). A temporal bone computed tomography (CT) scan revealed complete opacification of the left mesotympanum, retrotympanum, epitympanum, and aditus ad antrum, with no evidence of ossicular chain erosion, scutum erosion, or tegmen tympani dehiscence (Figure 2).
Surgical exploration via left tympanomastoidectomy was performed, revealing a polypoid mass with an epithelial layer occupying the mastoid antrum, aditus ad antrum, retrotympanum, mesotympanum, and hypotympanum. The ossicular chain was surrounded by this mass and was found to be disrupted, with the long process of the incus absent. The characteristics of the mass did not align with common differential diagnoses such as cholesteatoma, facial nerve neuroma, encephalocele, granulation tissue, or a high-riding jugular bulb. An incisional biopsy was performed for further evaluation.
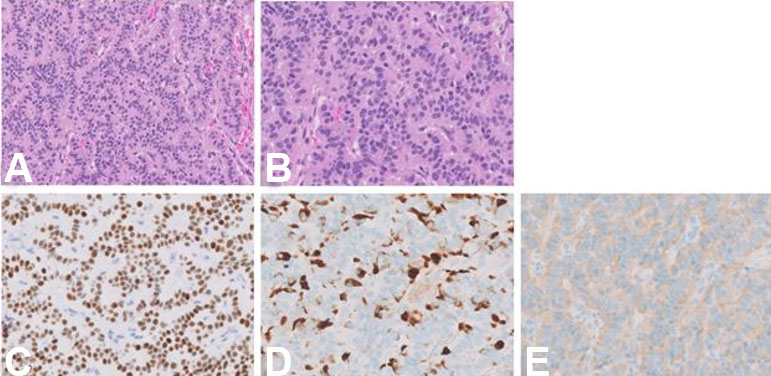
Histopathological analysis of the specimen revealed duct-like structures in a back-to-back configuration, lined by cuboidal to columnar cells with eosinophilic cytoplasm and bland ovoid nuclei. Immunohistochemistry demonstrated tumor cells positive for AE1/AE3, synaptophysin, chromogranin, vimentin, and INSM1. The Ki-67 proliferation index was 1–2%. These findings were consistent with a grade 1 neuroendocrine tumor (Figure 3).
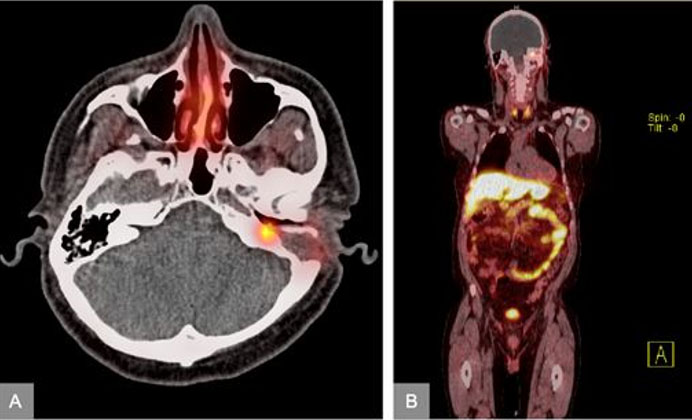
At the first postoperative visit, the patient reported additional symptoms experienced over the past two years, including unexplained episodes of tachycardia, flushing, diarrhea, diaphoresis, and chest pain. A subsequent positron emission tomography and computed tomography (PET/CT) scan revealed increased metabolic activity in the left middle ear, consistent with the known neuroendocrine tumor (Figure 4).
A revision canal wall up mastoidectomy was performed, successfully achieving near-total removal of the middle ear and mastoid mass due to tumor extension into the oval window.
Discussion
Middle ear neuroendocrine tumors are low-grade malignant lesions with rare local recurrences and distant metastases. They typically present in the fifth decade of life and affect both sexes equally. The most common presenting symptom is unilateral conductive hearing loss, reported in 86% of patients [6]. Other reported symptoms include otalgia, otorrhea, tinnitus, and aural fullness [6],[7],[8]. Facial nerve paralysis may occur, likely due to neural compression rather than perineural invasion [9].
Neuroendocrine tumors, in general, are classified as functioning or non-functioning based on the presence of tumor-specific syndromes [10]. Functioning neuroendocrine tumors are associated with the secretion of bioactive substances, leading to clinical syndromes such as carcinoid syndrome, which is characterized by flushing and diarrhea [10]. The case presented here is the first reported instance of a functioning MeNET, adding a new dimension to the clinical understanding of these tumors.
On otoscopic examination, MeNETs typically appear as retrotympanic brownish-red masses with an intact tympanic membrane [4]. Computed tomography scans usually reveal a homogenous, hypodense mass limited to the middle ear, often showing bone invasion, encasement of the ossicles, and associated bone remodeling without significant destruction [4]. Magnetic resonance imaging (MRI) findings typically include an iso-intense mass in T1 with homogenous enhancement following the injection of gadolinium [11].
Histologically, MeNETs predominantly exhibit duct-like structures arranged in a back-to-back gland configuration. Immunohistochemistry plays a crucial role in diagnosing MeNETs; staining for chromogranin A, synaptophysin, and CD56 is necessary to confirm the histopathologic diagnosis [1]. The Ki-67 proliferation index and mitotic count are required for MeNET grading, prognosis, and therapeutic decision-making [12].
The primary treatment for MeNETs is complete surgical resection, often requiring removal of the ossicles [4]. Most tumors are excised in a piecemeal fashion [4], and 15–20% of patients develop recurrence [9],[13]. Although uncommon, there have been case reports of patients with cervical lymph node involvement and distant metastasis [13],[14],[15],[16].
Following surgical resection, long-term follow-up is essential due to slow tumor progression and challenges in achieving complete resection with wide surgical margins [17]. Contrast-enhanced MRI is the preferred modality for ongoing surveillance [18].
Conclusion
Middle ear neuroendocrine tumors are exceedingly rare neoplasms with an indolent course and nonspecific clinical presentation. This case report represents the first documented instance of a functioning MeNET, expanding the current clinical understanding of these tumors by demonstrating their potential to produce systemic symptoms consistent with neuroendocrine activity. It underscores the importance of thorough clinical evaluation and increased awareness of MeNETs, as well as the need for continued research into their pathophysiology, management strategies, and long-term outcomes.
REFERENCES
1.
Katabi N. Neuroendocrine neoplasms of the ear. Head Neck Pathol 2018;12(3):362–6. [CrossRef]
[Pubmed]

2.
Hyams VJ, Michaels L. Benign adenomatous neoplasm (adenoma) of the middle ear. Clin Otolaryngol Allied Sci 1976;1(1):17–26. [CrossRef]
[Pubmed]
3.
Murphy GF, Pilch BZ, Dickersin GR, Goodman ML, Nadol JB Jr. Carcinoid tumor of the middle ear. Am J Clin Pathol 1980;73(6):816–23. [CrossRef]
[Pubmed]
4.
Bell D, El-Naggar AK, Gidley PW. Middle ear adenomatous neuroendocrine tumors: A 25-year experience at MD Anderson Cancer Center. Virchows Arch 2017;471(5):667–72. [CrossRef]
[Pubmed]
5.
Marinelli JP, Cass SP, Mann SE, Haynes DS, Hunter JB, Isaacson B, et al. Adenomatous neuroendocrine tumors of the middle ear: A multi-institutional investigation of 32 cases and development of a staging system. Otol Neurotol 2018;39(8):e712–21. [CrossRef]
[Pubmed]
6.
Pelosi S, Koss S. Adenomatous tumors of the middle ear. Otolaryngol Clin North Am 2015;48(2):305–15. [CrossRef]
[Pubmed]
7.
Ratnayake GM, Luong TV, Toumpanakis C, Caplin M, Grossman AB. Middle ear neuroendocrine tumours: Insight into their pathogenesis, diagnosis and management. J Neuroendocrinol 2021;33(9):e13031. [CrossRef]
[Pubmed]
8.
Bruschini L, Canelli R, Cambi C, Fiacchini G, Berrettini S, Forli F. Middle ear neuroendocrine adenoma: A case report and literature review. Case Rep Otolaryngol 2020;2020:8863188. [CrossRef]
[Pubmed]
9.
Torske KR, Thompson LDR. Adenoma versus carcinoid tumor of the middle ear: A study of 48 cases and review of the literature. Mod Pathol 2002;15(5):543–55. [CrossRef]
[Pubmed]
10.
Marasco M, Romano E, Arrivi G, Prosperi D, Rinzivillo M, Caruso D, et al. Exploring carcinoid syndrome in neuroendocrine tumors: Insights from a multidisciplinary narrative review. Cancers (Basel) 2024;16(22):3831. [CrossRef]
[Pubmed]
11.
Abrahão NM, Guimarães GC, Tamanini JB, de Oliva Costa SF, de Mesquita Ferreira PJ, da Silva VAR, et al. Neuroendocrine adenoma of middle ear: A case report and endoscopic approach. Braz J Otorhinolaryngol 2024;90(4):101432. [CrossRef]
[Pubmed]
12.
Niewiadomska A, Graźyńska A, Barczyk-Gutkowska A, Ludwik K, Kuźbińska A, Steinhof-Radwańska K. Neuroendocrine tumor of the middle ear. Pol Arch Intern Med 2024;134(6):16732. [CrossRef]
[Pubmed]
13.
Ramsey MJ, Nadol JB Jr, Pilch BZ, McKenna MJ. Carcinoid tumor of the middle ear: Clinical features, recurrences, and metastases. Laryngoscope 2005;115(9):1660–6. [CrossRef]
[Pubmed]
14.
Pellini R, Ruggieri M, Pichi B, Covello R, Danesi G, Spriano G. A case of cervical metastases from temporal bone carcinoid. Head Neck 2005;27(7):644–7. [CrossRef]
[Pubmed]
15.
Fundakowski CE, Chapman JR, Thomas G. Middle ear carcinoid with distant osseous metastasis. Laryngoscope 2013;123(3):779–82. [CrossRef]
[Pubmed]
16.
Gaafar A, Ereño C, Ignacio López J, Fernández de Larrinoa A, Grande J, Salazar J, et al. Middle-ear carcinoid tumor with distant metastasis and fatal outcome. Hematol Oncol Stem Cell Ther 2008;1(1):53–6. [CrossRef]
[Pubmed]
17.
Xie B, Zhang S, Dai C, Liu Y. Middle ear adenomatous neuroendocrine tumors: Suggestion for surgical strategy. Braz J Otorhinolaryngol 2022;88(1):83–8. [CrossRef]
[Pubmed]
18.
Zwierz A, Masna K, Burduk P. Preoperative diagnosis and treatment of middle ear adenoma: A case report and literature review. Ear Nose Throat J 2021;100(3_suppl):360S–3S. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Natasha JMinaya - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nirmal Thapa - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Natasha J Minaya et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



