 |
Case Report
Diagnostic pitfalls in primary Eustachian tube squamous cell carcinoma initially managed as chronic otitis media: A case report
1 Project Assistant Professor, Department of Head and Neck Surgery, Institute of Science Tokyo, Tokyo, Japan
2 Assistant Professor, Department of Head and Neck Surgery, Institute of Science Tokyo, Tokyo, Japan
3 Junior Associate Professor, Department of Otorhinolaryngology, Institute of Science Tokyo, Tokyo, Japan
4 Professor, Department of Otorhinolaryngology, Institute of Science Tokyo, Tokyo, Japan
5 Professor, Department of Head and Neck Surgery, Institute of Science Tokyo, Tokyo, Japan
Address correspondence to:
Tomoaki Asamori
Department of Head and Neck Surgery, Institute of Science Tokyo, 1-5-45 Yushima, Bunkyo-ku, Tokyo 113-8519,
Japan
Message to Corresponding Author
Article ID: 100019Z18TA2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Asamori T, Okada R, Ito T, Tsutsumi T, Asakage T. Diagnostic pitfalls in primary Eustachian tube squamous cell carcinoma initially managed as chronic otitis media: A case report. J Case Rep Images Otolaryngol 2026;5(1):1–5.ABSTRACT
Introduction: Primary squamous cell carcinoma (SCC) of the Eustachian tube (ET) is an extremely rare and difficult to diagnose because of its deep anatomical location and nonspecific otologic symptoms. In addition, routine temporal bone computed tomography (CT) does not always visualize the entire ET, which can contribute to diagnostic delay.
Case Report: A 53-year-old male presented with a two-year history of unilateral ear fullness and progressive conductive hearing loss without otorrhea, otalgia, or ear bleeding. He was initially treated for otitis media with effusion (OME) with tympanostomy tube placement and subsequently underwent tympanoplasty with canal wall-up mastoidectomy for suspected cholesteatoma at a tertiary care hospital. Histopathological examination of granulation tissue initially revealed inverted papilloma (IP), but pathological review at our hospital led to a diagnosis of SCC. Endoscopic examination revealed a mass at the pharyngeal orifice of the ET, and subsequent imaging studies demonstrated a tumor extending along the course of the ET. Definitive chemoradiotherapy resulted in complete remission, and the patient remains disease-free five years after treatment.
Conclusion: This case illustrates the diagnostic difficulty of ET carcinoma presenting as prolonged unilateral OME. When the clinical course is atypical or prolonged, disease beyond the middle ear should be considered, and assessment of the ET and nasopharynx with appropriate imaging and endoscopic evaluation may help prevent delayed diagnosis.
Keywords: Diagnostic imaging, Eustachian tube carcinoma, Inverted papilloma, Squamous cell carcinoma
Introduction
Primary carcinoma of the Eustachian tube (ET) is exceptionally rare, accounting for only a minute fraction of head and neck cancers. A systematic review identified 78 reported cases of primary ET tumors and tumor-like lesions, including malignant lesions, of which 18 were carcinomas [1],[2],[3],[4]. Because of its deep anatomical location and nonspecific symptoms such as ear fullness or hearing loss, early diagnosis is often difficult. In addition, standard temporal bone CT may not adequately visualize the ET, making radiological evaluation challenging.
We report a rare case of ET squamous cell carcinoma (SCC), emphasizing the diagnostic difficulties and the importance of meticulous radiological and pathological evaluation.
Case Report
A 53-year-old Sri Lankan male presented with a two-year history of left ear fullness and progressive hearing loss, without otorrhea, otalgia, or ear bleeding. He initially visited a local ear, nose, and throat (ENT) clinic and was diagnosed with left otitis media with effusion (OME). Despite tympanostomy tube placement, his symptoms did not improve and his hearing gradually worsened. He was therefore referred from the local ENT clinic to a tertiary care hospital, where cholesteatoma was suspected based on temporal bone CT, and surgical treatment was planned.
Medical history: Lumbar disc herniation (surgically treated at age 40)
Alcohol consumption: Beer 350 mL/day (positive alcohol flush reaction)
Smoking: None
Examination Findings at the Referring Hospital
Tympanic membrane findings: A tympanostomy tube was observed in the left tympanic membrane, with serous effusion discharge.
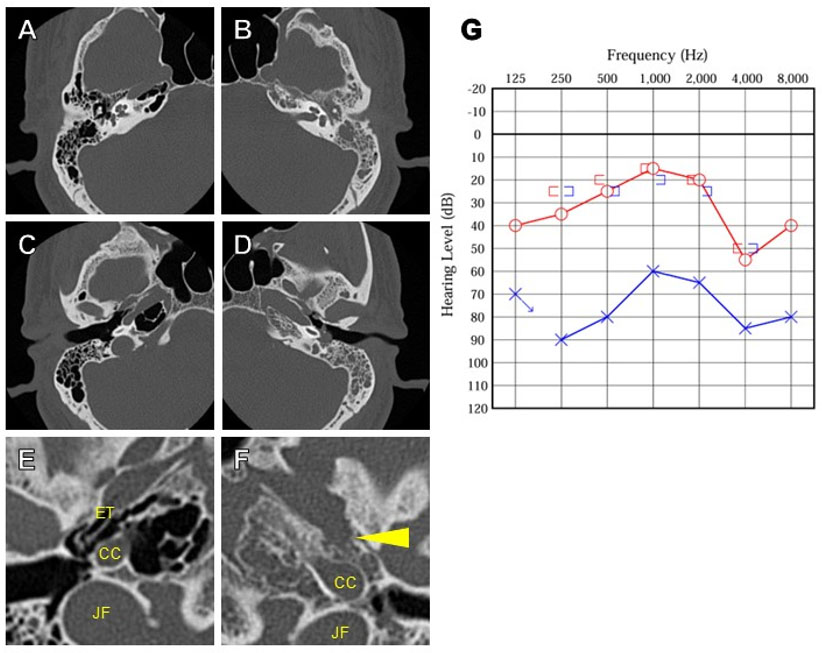
Temporal bone CT: Figure 1A, Figure 1B, Figure 1C, Figure 1D, Figure 1E, Figure 1F.
Pure-tone audiometry showed severe conductive hearing loss on the left (four-frequency average 66.3 dB) and normal hearing on the right (18.8 dB) (Figure 1G).
Based on these findings, the patient underwent tympanoplasty with canal wall-up mastoidectomy at the referring hospital. Intraoperatively, extensive, friable granulation tissue extended from the entire tympanic cavity to the mastoid antrum, with erosion of the incus long process. A remnant tympanostomy tube was found in the anterior mesotympanum, likely contributing to the granulation tissue proliferation. The facial nerve was not exposed intraoperatively. Initial pathological examination revealed inverted papilloma (IP); however, the diagnosis was revised to SCC at our hospital, and the patient was referred to our institution for further management.
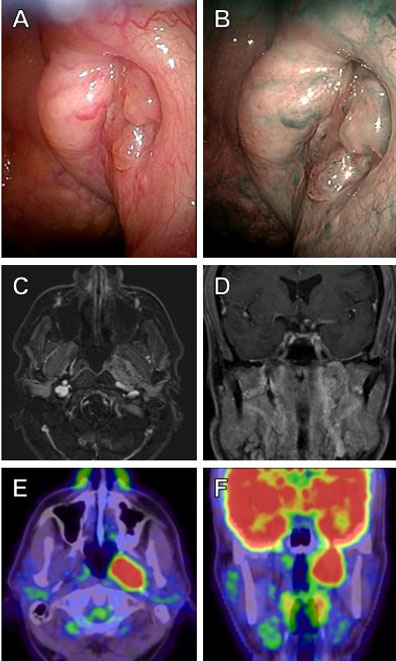
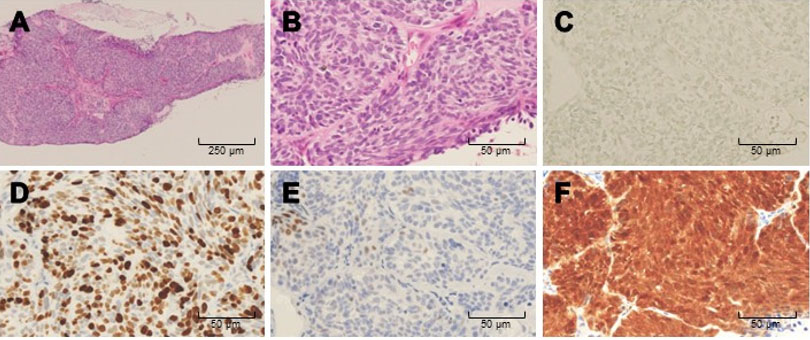
At the initial visit to our hospital, a tumor was observed at the pharyngeal orifice of the ET (Figure 2A and Figure 2B). Magnetic resonance imaging (MRI) revealed a 34 mm enhancing lesion along the ET (Figure 2C and Figure 2D), with corresponding FDG uptake on PET-CT (Figure 2E and Figure 2F). Biopsy from the tumor at the pharyngeal opening also confirmed SCC (Figure 3). Radical chemoradiotherapy (CDDP 100 mg/m2 × three times, RT S60 Gy) led to complete remission without grade 3 or higher toxicity. The patient remains disease-free at five years, and tympanoplasty was later performed for residual perforation.
Discussion
This case represents an exceedingly rare malignancy originating from the ET, a site that is seldom involved in head and neck cancers. The clinical challenges of accurately diagnosing the tumor and identifying its site of origin, as well as the suspected malignant transformation from IP, are notable features.
Tumor Origin and Diagnostic Considerations
Most reported ET carcinomas are histologically SCC or non-keratinizing carcinoma (formerly called transitional cell carcinoma) [1],[2],[3],[4]. The ET, approximately 3.5 cm in length, connects the nasopharynx to the middle ear and is lined with ciliated columnar epithelium. The nasopharyngeal mucosa comprises stratified squamous, ciliated columnar, and transitional epithelium, whereas the middle ear is predominantly lined by columnar epithelium. Ciliated columnar epithelium is known to undergo squamous metaplasia under chronic inflammatory conditions, which may contribute to carcinogenesis.
In this case, SCC was identified at both the pharyngeal and tympanic orifices of the ET, and EBER-ISH was negative (Figure 3C), unlike nasopharyngeal carcinoma where EBV association is frequent [5]. Imaging demonstrated a lesion following the ET course without clear predominance toward either the nasopharynx or middle ear (Figure 2C), making the primary site indeterminate. Future molecular analyses may help elucidate the epithelial origin of such tumors.
Malignant Transformation of Inverted Papilloma
Primary IP of the middle ear is extremely rare, with recurrence and malignant transformation rates (53.8% and 38.5%) exceeding those of sinonasal IPs (5–27%) [6],[7],[8]. Because many cases of middle ear IP coexist with sinonasal IP, a nasopharyngeal origin was also considered in the present case.
Immunohistochemically, p16 expression has been reported in 18–55% of IPs [8],[9], although its correlation with human papillomavirus (HPV) DNA remains relatively low [10]. Diffuse p16 positivity was observed in this case; however, p16 overexpression is not specific for HPV-driven carcinogenesis and may also reflect reactive changes associated with chronic inflammation or non-HPV-related pathways [11]. As HPV DNA testing was not performed, the role of HPV in the present tumor cannot be determined.
Challenges in Radiological Diagnosis
In standard temporal bone CT protocols, the imaging field usually spans from approximately 1 cm superior to the petrous apex to the mastoid tip, generally including the ET. However, some institutions limit the scanning range or upload only bone-window images, reducing diagnostic accuracy.
In the present case, a subtle bony destruction anterior to the petrous apex was identifiable only in retrospect on the pre-treatment CT; however, recognizing this as indicative of ET carcinoma would have been extremely difficult at the time. Even in candidates for otologic surgery, evaluation should extend beyond the temporal bone to include the petrous apex and the entire ET. In addition to high-resolution CT—carefully inspected for subtle bony destruction—contrastenhanced MRI and, when indicated, nasopharyngoscopy may help detect lesions at the pharyngeal orifice of the ET that can be overlooked when the clinical focus is primarily on middle ear disease. The lack of nasopharyngoscopic evaluation before ear surgery may also have contributed to delayed detection of this lesion.
Conclusion
Primary SCC of the ET is rare and may present with nonspecific otologic symptoms, leading to delayed diagnosis. In this case, the tumor extended along the course of the ET and was difficult to detect on routine preoperative imaging focused on the middle ear. When unilateral OME is prolonged and even subtle abnormal findings are present preoperatively, disease involvement beyond the middle ear, including ET and nasopharynx, should be considered. Careful review of temporal bone CT, together with contrast-enhanced MRI and nasopharyngoscopy when appropriate, may help avoid missing this rare entity.
REFERENCES
1.
Muzzi E, Cama E, Boscolo-Rizzo P, Trabalzini F, Arslan E. Primary tumors and tumor-like lesions of the Eustachian tube: A systematic review of an emerging entity. Eur Arch Otorhinolaryngol 2012;269(7):1723–32. [CrossRef]
[Pubmed]

2.
le Nobel GJ, Lin VY, Iakovlev V, Lee JM. An Eustachian tube neuroendocrine carcinoma: A previously undescribed entity and review of the literature. Case Rep Surg 2016;2016:4643615. [CrossRef]
[Pubmed]
3.
Yoon WY, Massoud TF. External auditory canal involvement by nasopharyngeal carcinoma via Eustachian tube spread: A case report. Radiol Case Rep 2024;19(10):4604–9. [CrossRef]
[Pubmed]
4.
Nacouzi M, El-Amine R, Sakr R, Yazbeck S, Rohayem Z. Cystic lesion of the Eustachian tube: Pathology and management of a rare case presentation. J Clin Case Rep 2020;10:1352.
5.
Su ZY, Siak PY, Leong CO, Cheah SC. The role of Epstein-Barr virus in nasopharyngeal carcinoma. Front Microbiol 2023;14:1116143. [CrossRef]
[Pubmed]
6.
Kainuma K, Kitoh R, Kenji S, Usami SI. Inverted papilloma of the middle ear: A case report and review of the literature. Acta Otolaryngol 2011;131(2):216–20. [CrossRef]
[Pubmed]
7.
Stepp WH, Farzal Z, Kimple AJ, Ebert CS Jr, Senior BA, Zanation AM, et al. HPV in the malignant transformation of sinonasal inverted papillomas: A meta-analysis. Int Forum Allergy Rhinol 2021;11(10):1461–71. [CrossRef]
[Pubmed]
8.
Rha MS, Kim CH, Yoon JH, Cho HJ. Association of the human papillomavirus infection with the recurrence of sinonasal inverted papilloma: A systematic review and meta-analysis. Rhinology 2022;60(1):2–10. [CrossRef]
[Pubmed]
9.
Jenko K, Kocjan B, Zidar N, Poljak M, Strojan P, Zargi M, et al. In inverted papillomas HPV more likely represents incidental colonization than an etiological factor. Virchows Arch 2011;459(5):529–38. [CrossRef]
[Pubmed]
10.
Scheel A, Lin GC, McHugh JB, Komarck CM, Walline HM, Prince ME, et al. Human papillomavirus infection and biomarkers in sinonasal inverted papillomas: Clinical significance and molecular mechanisms. Int Forum Allergy Rhinol 2015;5(8):701–7. [CrossRef]
[Pubmed]
11.
Becker AS, Merkel J, Bozkurt I, Strüder DF, Maletzki C, Hühns M, et al. p16 overexpression identifies oncogenic high-risk HPV infection in non-oropharyngeal squamous cell carcinoma of the head and neck. Head Neck 2024;46(10):2569–81. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
During the preparation of this manuscript, the authors used generative AI tools, ChatGPT (version GPT-5.2, OpenAI, CA, USA), for language editing and improving clarity of expression. All content was reviewed and edited by the authors, who take full responsibility for the accuracy and integrity of the final manuscript.
Author ContributionsTomoaki Asamori - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ryuhei Okada - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Taku Ito - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Takeshi Tsutsumi - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Takahiro Asakage - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Tomoaki Asamori et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



