 |
Case Report
In vivo and ex vivo interrogation of the spectral properties of a middle ear and mastoid cholesteatoma
1 MD, Physician, Department of Otolaryngology, New York University Langone Health, New York, NY, USA
2 MD, Physician, Department of Radiology, New York University Langone Health, New York, NY, USA
3 Senior Staff Scientist, Siemens Healthineers, Malvern, PA 19355, USA
4 Medical Student, Department of Otolaryngology, New York University Langone Health, New York, NY, USA
5 MD, Physician, Department of Pathology, New York University Langone Health, New York, NY, USA
6 MD, Department of Radiology, New York University Langone Health, New York, NY, USA
Address correspondence to:
Justin Cottrell
MD, Department of Otolaryngology, NYU Langone Medical Center, 550 First Avenue, New York, NY 10010,
USA
Message to Corresponding Author
Article ID: 100020Z18JC2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cottrell J, Dogra S, O’Donnell T, Scudder M, Liu CZ, McMenomey S, Jethanamest D, Moonis G. In vivo and ex vivo interrogation of the spectral properties of a middle ear and mastoid cholesteatoma. J Case Rep Images Otolaryngol 2026;5(1):6–11.ABSTRACT
Introduction: We sought to compare in vivo and ex vivo spectral properties of a recurrent middle ear and mastoid cholesteatoma.
Case Report: A 25-year-old male with clinically suspected recurrent cholesteatoma four years after a canal wall up mastoidectomy was consented for the study. He underwent preoperative computed tomography (CT) imaging of the temporal bone on a Photon Counting CT scanner followed by right tympanomastoidectomy with cholesteatoma removal. The cholesteatoma specimen was separated into mastoid and middle ear samples that were packed in two centrifuge tubes and placed in a phantom to scan on a dual energy computed tomography (DECT) scanner. Following post-processing, regions-of-interest (ROIs) were placed on pre- and post-operative images and iodine densities were compared. On in vivo images, iodine densities were 0.9 mg/mL in a mastoid ROI, 0.3 mg/mL in an aditus ad antrum ROI, −0.7 mg/mL in a middle ear ROI and 0 mg/mL in a right cerebellar ROI (used as reference). On ex vivo images, iodine densities were 0.1 mg/mL in both the mastoid and tympanic specimens.
Conclusion: In vivo cholesteatoma iodine densities differed based on location. The mastoid iodine density was higher than ex vivo cholesteatoma iodine densities, which may reflect a combination of beam hardening artifact on in vivo images, sample rinsing before transfer to the centrifuge tubes, and different scanners used for in vivo and ex vivo images. Additional research is needed to better understand variations in in vivo and ex vivo findings to facilitate accurate dual energy spectral analysis.
Keywords: Cholesteatoma, Dual energy, Photon counting, Spectral properties
Introduction
Cholesteatomas are collections of keratin debris, a perimatrix consisting of subepithelial connective tissue of varying thickness, and matrix lining of stratified squamous epithelium located most often within the middle ear and mastoid bone [1],[2]. Bone resorption in areas adjacent to a cholesteatoma is common, resulting from recurrent infections and inflammatory reactions [2]. They are most commonly classified into congenital and acquired categories, reflecting differences in underlying etiology [2]. While both categories differ in terms of clinical presentation and location, surgical excision remains the mainstay of treatment for both [2],[3]. Imaging is not required for diagnosis; however, it can provide important insight into disease extent and severity to facilitate pre-operative planning and detection of recurrence [2].
Magnetic resonance imaging (MRI), particularly diffusion-weighted imaging (DWI), is more specific for the diagnosis of cholesteatoma than computed tomography (CT) and better differentiates residual and recurrent cholesteatoma from granulation tissue in post-operative patients [4],[5]. However, MRI has less utility for surgical planning due to limited bone detail [6]. Undergoing both MRI and CT may delay management and increase costs. Computed tomography, despite having high sensitivity for soft tissue density in the middle ear, continues to struggle differentiating cholesteatoma from granulation tissue and cholesterol granulomas [6].
Prior investigations of CT characteristics differentiating cholesteatoma from these other soft tissue densities have had mixed results. A difference in Hounsfield units between cholesteatoma and inflammatory granulation tissue in the mastoid antrum has been described; however, this has not been replicated in other studies [7],[8],[9]. With the advent of dual energy CT (DECT) scanners, spectral analysis and material decomposition have been proposed as new methods for evaluating cholesteatoma [10]. A study using DECT to evaluate residual or recurrent cholesteatoma found significantly different Hounsfield units between positive and negative cases [5]. More recently, photon-counting CT (PCCT) offers numerous additional benefits to DECT, including increased spatial resolution, and also enables spectral analysis by quantifying the energy level of each photon [11],[12],[13].
No study thus far has compared the in vivo and ex vivo spectral properties of the same sample of cholesteatoma. These comparisons have important implications such as validation of pre-operative spectral signatures to pathology-proven cholesteatoma, understanding potential post-extraction biochemical changes that alter spectral qualities, and protocol standardization. The purpose of our study was to compare in vivo and ex vivo spectral properties of a middle ear and mastoid cholesteatoma, hypothesizing that properties would be similar between the in vivo and ex vivo states.
Case Report
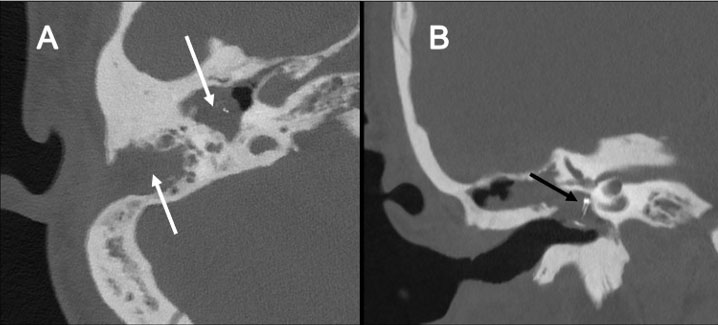
This study was approved by our Institutional Review Board (IRB# I23-00196). A 25-year-old male with hearing loss and intermittent otorrhea was found to have a cholesteatoma and underwent canal wall up tympanomastoidectomy, ossicular chain reconstruction with a hydroxyapatite total ossicular reconstruction prosthesis, and cartilage graft. He subsequently developed recurrent otorrhea and evidence of recidivistic disease on examination. Prior to revision surgery, pre-operative imaging was performed on a Siemens Healthineers NAEOTOM Alpha photon-counting scanner (Forchheim, Germany). The scan mode was Spiral Adult Head Highresultra Quantumplus at 140 kV, image quality (IQ) level 201 with a CT dose index (CTDI) of 57.8 mGy (16 cm phantom) and a dose length product (DLP) of 577 mGy*cm. The rotation time was 0.5 and the pitch was 0.85. The images were reconstructed with a Qr76 kernel at quantum iterative reconstruction (QIR) strength 3, slice thickness 0.4 mm in spectral post-processing (SPP) mode. Imaging findings supported a clinical diagnosis of cholesteatoma (lobulated soft tissue mass in the mastoid and middle ear with osseous erosion), and the patient was consented for surgery as well as inclusion in this study (Figure 1).
The patient underwent a right tympanomastoidectomy, which confirmed extensive cholesteatoma in the middle ear and mastoid. The cholesteatoma was excised and the specimens (tympanic and mastoid) were rinsed with saline to remove blood products, then separately placed into two 2 mL centrifuge tubes. The tubes were placed in a custom slotted phantom QRM (Möhrendorf, Germany), and scanned on a Siemens Healthineers SOMATOM Force using a dual energy protocol (80/Sn150 kV) at (1500/750 mAs) with a CTDI of 53.87 mGy and a DLP of 603.3 mGy*cm. The rotation time was 0.5 s and the pitch was 0.3. Following imaging, samples were placed in formalin and delivered to pathology for analysis. The sample images were reconstructed with a Qr44 kernel QIR strength 4, slice thickness 0.5 mm in SPP mode.
The reconstructed in vivo and ex vivo images were post-processed using Syngo Via version VB60 with the Dual Energy workflow, Virtual Unenhanced application. These were non-contrast scans so no iodine was introduced. However, the Virtual Unenhanced application’s iodine concentration parameter was used as a convenient proxy for material characterization. Regions-of-interest (ROIs) were placed on pre- and post-operative axial slices following the aforementioned post-processing.
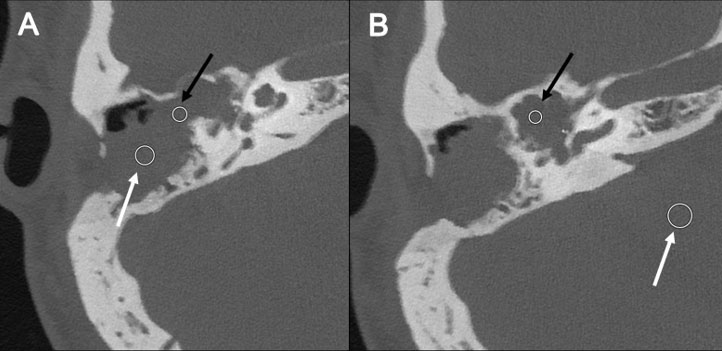
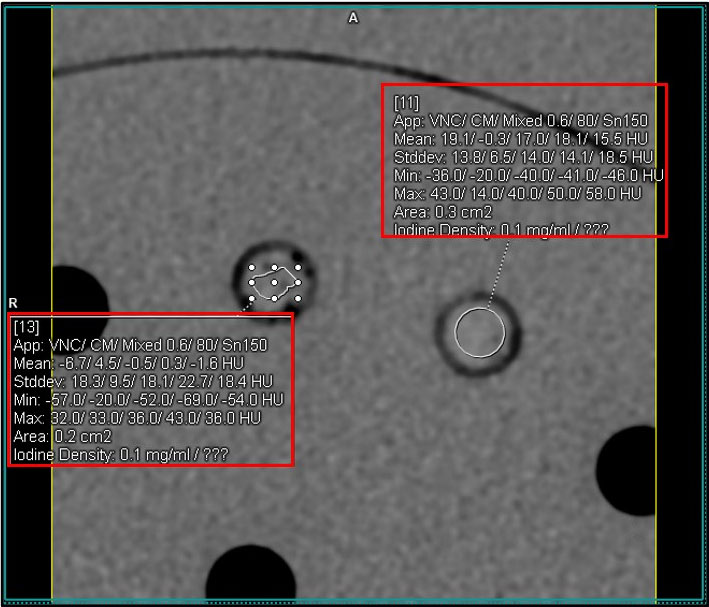
On preoperative imaging, as the cholesteatoma was found to extend from the middle ear to the mastoid, one ROI was placed in the mastoid, one in the aditus ad antrum and one in the middle ear on axial slices (Figure 2). Another ROI was placed in the cerebellum as a control. Regions-of-interest were placed away from the margins to avoid areas of possible neo-ossification. For post-operative imaging, one ROI was placed on each of the samples contained in the centrifuge tubes, also on an axial slice (Figure 3). Iodine density was recorded for each ROI.
Pathologic evaluation of both specimens returned keratotic material, fragments of keratinizing squamous epithelium, mixed inflammatory debris, fibrous tissue, and osseous tissue confirming a diagnosis of cholesteatoma.
Regions-of-interest were placed on preoperative axial slices as described (Figure 2). Iodine densities were 0.9 mg/mL in the mastoid ROI, 0.3 mg/mL in the aditus ad antrum ROI, –0.7 mg/mL in the middle ear ROI, and 0 mg/mL in a right cerebellar ROI (used as reference).
Regions-of-interest were also placed on an axial slice obtained from imaging of a phantom containing two tubes, which contained separate mastoid and tympanic intraoperative samples (Figure 3). Regions-of-interest from both samples had iodine densities of 0.1 mg/mL.
Discussion
In recent years, with the growing popularity of DECT and now PCCT, spectral imaging techniques have been increasingly applied to several clinical use cases, ranging from uric acid crystals in gout to kidney stones [14],[15],[16],[17],[18],[19]. Numerous types of spectral data can be obtained, such as iodine density, electron density, and effective atomic number [20]. By enabling improved separation of tissues with differing material properties that have similar densities, spectral imaging has the potential to increase the sensitivity of CT for distinguishing cholesteatoma from other entities commonly encountered in the pathologic middle ear, such as granulation tissue, and may decrease the need for second-look surgeries [21]. To our knowledge, no prior study has investigated the spectral properties of cholesteatoma. Moreover, this study is the first to present a comparative analysis of in vivo and ex vivo spectral properties of middle ear and mastoid cholesteatoma specimens.
Our results demonstrate different in vivo and ex vivo cholesteatoma iodine densities. Additionally, there was heterogeneity in the iodine density of the cholesteatoma with different spectral values between the components in the mastoid air cell, aditus ad antrum and the middle ear cavity. The mastoid pre-operative ROIs had an iodine density of 0.9 mg/mL while both the post-operative mastoid and tympanic samples had lower iodine densities of 0.1 mg/mL. Interestingly, the antrum ROI iodine density was in between these two values, at 0.5 mg/mL and the ROI in the middle ear showed –0.7 mg/mL. The lower iodine density of the antrum and middle ear soft tissue compared with mastoid soft tissue may reflect differences in cholesteatoma histology, including cholesterol deposition resulting in lower density, beam hardening artifact from the ossicular reconstruction prosthesis in the middle ear, and bone resorption byproducts in the mastoid contributing to higher density. The cerebellar ROI used as a reference demonstrated no measurable iodine density.
The discrepancy between in vivo and ex vivo results warrants further study, and may be attributable to variables such as image artifact, preparation technique, CT scan type, among others. Beam hardening can occur as x-rays travel through the skull, which may contribute to higher iodine densities of in vivo images [22]. In addition to beam hardening, sample preparation utilizing a saline rinse could also impact composition and thus iodine density. The decision to rinse specimens before placement into the centrifuge tube was made due to the concern of residual blood from surgical extraction confounding results. Pathologic assessment did not reveal degradation or abnormality of the specimen; however chemical changes could still have occurred. The methodology utilized in this study suggests that cholesteatoma specimens can undergo imaging between surgical extraction and pathologic fixation without evidence of degradation that would compromise accurate pathologic diagnosis. As noted in the methods, the scanner varied, with in vivo imaging performed utilizing a photon-counting detector CT, and ex vivo imaging performed on a dual-source CT. While spectral analysis can be performed with both technologies, it is possible that a very slight variability in calculated iodine density could be introduced as a result of technical differences [23].
Spectral analysis, particularly within the temporal bone, is still in its infancy. These preliminary findings are derived from a single patient, and may not generalize to all patients and workflows. It does demonstrate however that expected in vivo and ex vivo spectral analysis may not be concordant. This impacts the ability to infer characteristic iodine density values to cholesteatoma, until variables that result in these differences can be identified and mitigated. It is of interest whether spectral analysis of material within the skull may be impacted by the surrounding bone [24]. Even in the presence of artifact, novel means of differentiating cholesteatoma from other temporal bone tissue may be feasible utilizing multiple ROI sampling of areas such as Prussak’s space and the epitympanum to see if exclusive signatures emerge.
Conclusion
This case highlights spectral analysis from a single patient with recidivistic acquired cholesteatoma. Preliminary findings demonstrate that in vivo and ex vivo results may differ. Drivers of these differences should be a focus moving forward to better understand the implications in each setting which can then facilitate accurate large-scale studies.
REFERENCES
1.
Castle JT. Cholesteatoma pearls: Practical points and update. Head Neck Pathol 2018;12(3):419–29. [CrossRef]
[Pubmed]

2.
Yung M, Tono T, Olszewska E, Yamamoto Y, Sudhoff H, Sakagami M, et al. EAONO/JOS Joint Consensus Statements on the definitions, classification and staging of middle ear cholesteatoma. J Int Adv Otol 2017;13(1):1–8. [CrossRef]
[Pubmed]
3.
Kuo CL, Liao WH, Shiao AS. A review of current progress in acquired cholesteatoma management. Eur Arch Otorhinolaryngol 2015;272(12):3601–9. [CrossRef]
[Pubmed]
4.
Allam HS, Abdel Razek AAK, Ashraf B, Khalek M. Reliability of diffusion-weighted magnetic resonance imaging in differentiation of recurrent cholesteatoma and granulation tissue after intact canal wall mastoidectomy. J Laryngol Otol 2019;133(12):1083–6. [CrossRef]
[Pubmed]
5.
Foti G, Beltramello A, Minerva G, Catania M, Guerriero M, Albanese S, et al. Identification of residual-recurrent cholesteatoma in operated ears: Diagnostic accuracy of dual-energy CT and MRI. Radiol Med 2019;124(6):478–86. [CrossRef]
[Pubmed]
6.
Manik S, Dabholkar Y, Bhalekar S, Velankar H, Chordia N, Saberwal A. Sensitivity and specificity of high-resolution computed tomography (HRCT) of temporal bone in diagnosing cholesteatoma and its correlation with intraoperative findings. Indian J Otolaryngol Head Neck Surg 2021;73(1):25–29. [CrossRef]
[Pubmed]
7.
Park MH, Rah YC, Kim YH, Kim JH. Usefulness of computed tomography Hounsfield unit density in preoperative detection of cholesteatoma in mastoid ad antrum. Am J Otolaryngol 2011;32(3):194–7. [CrossRef]
[Pubmed]
8.
Salepci E, Ugurlar M, Ucpinar BA, Gemalmaz A, Turgut S. Can Hounsfield unit density accurately predict recurrent cholestatoma in previously operated ears? J Coll Physicians Surg Pak 2021;31(1):104–6. [CrossRef]
[Pubmed]
9.
Lee DH, Kim CS, Park CW, Chung DY. Is preoperative computed tomographic density measurement of soft tissues helpful in the diagnosis of cholesteatoma? Ann Otol Rhinol Laryngol 2012;121(12):792–7. [CrossRef]
[Pubmed]
10.
So A, Nicolaou S. Spectral computed tomography: Fundamental principles and recent developments. Korean J Radiol 2021;22(1):86–96. [CrossRef]
[Pubmed]
11.
Tortora M, Gemini L, D’Iglio I, Ugga L, Spadarella G, Cuocolo R. Spectral photon-counting computed tomography: A review on technical principles and clinical applications. J Imaging 2022;8(4):112. [CrossRef]
[Pubmed]
12.
Macielak RJ, Benson JC, Lane JI, Carlson ML, Leng S. Photon-counting detector CT for temporal bone imaging: Up to three times the resolution at half the radiation dose. Otol Neurotol 2022;43(10):e1205–7. [CrossRef]
[Pubmed]
13.
Takahashi Y, Higaki F, Sugaya A, Asano Y, Kojima K, Morimitsu Y, et al. Evaluation of the ear ossicles with photon-counting detector CT. Jpn J Radiol 2024;42(2):158–64. [CrossRef]
[Pubmed]
14.
Cheraya G, Sharma S, Chhabra A. Dual energy CT in musculoskeletal applications beyond crystal imaging: Bone marrow maps and metal artifact reduction. Skeletal Radiol 2022;51(8):1521–34. [CrossRef]
[Pubmed]
15.
Baffour FI, Ferrero A, Aird GA, Powell GM, Adkins MC, Bekele DI, et al. Evolving role of dual-energy CT in the clinical workup of gout: A retrospective study. AJR Am J Roentgenol 2022;218(6):1041–50. [CrossRef]
[Pubmed]
16.
Omoumi P, Becce F, Racine D, Ott JG, Andreisek G, Verdun FR. Dual-energy CT: Basic principles, technical approaches, and applications in musculoskeletal imaging (Part 1). Semin Musculoskelet Radiol 2015;19(5):431–7. [CrossRef]
[Pubmed]
17.
Primak AN, Fletcher JG, Vrtiska TJ, Dzyubak OP, Lieske JC, Jackson ME, et al. Noninvasive differentiation of uric acid versus non-uric acid kidney stones using dual-energy CT. Acad Radiol 2007;14(12):1441–7. [CrossRef]
[Pubmed]
18.
Ascenti G, Siragusa C, Racchiusa S, Ielo I, Privitera G, Midili F, et al. Stone-targeted dual-energy CT: A new diagnostic approach to urinary calculosis. AJR Am J Roentgenol 2010;195(4):953–8. [CrossRef]
[Pubmed]
19.
Boll DT, Patil NA, Paulson EK, Merkle EM, Simmons WN, Pierre SA, et al. Renal stone assessment with dual-energy multidetector CT and advanced postprocessing techniques: Improved characterization of renal stone composition—pilot study. Radiology 2009;250(3):813–20. [CrossRef]
[Pubmed]
20.
Greffier J, Villani N, Defez D, Dabli D, Si-Mohamed S. Spectral CT imaging: Technical principles of dual-energy CT and multi-energy photon-counting CT. Diagn Interv Imaging 2023;104(4):167–77. [CrossRef]
[Pubmed]
21.
Peña JA, Shaul JL, Müller M, Damm T, Barkmann R, Kurz B, et al. Dual-layer spectral-computed tomography enhances the separability of calcium-based implant material from bone: An ex vivo quantitative imaging study. J Bone Miner Res 2022;37(12):2472–82. [CrossRef]
[Pubmed]
22.
Cauley KA, Yorks PJ, Flora S, Fielden SW. The effects of the skull on CT imaging of the brain: A skull and brain phantom study. Br J Radiol 2021;94(1119):20200714. [CrossRef]
[Pubmed]
23.
Cai LM, Hippe DS, Zamora DA, Cao J, Parakh A, Kambadakone AR, et al. A method for reducing variability across dual-energy CT manufacturers in quantification of low iodine content levels. AJR Am J Roentgenol 2022;218(4):746–55. [CrossRef]
[Pubmed]
24.
Kanatani R, Shirasaka T, Kojima T, Kato T, Kawakubo M. Influence of beam hardening in dual-energy CT imaging: Phantom study for iodine mapping, virtual monoenergetic imaging, and virtual non-contrast imaging. Eur Radiol Exp 2021;5(1):18. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Justin Cottrell - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Siddhant Dogra - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Thomas O’Donnell - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Michael Scudder - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Cheng Z Liu - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sean McMenomey - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Daniel Jethanamest - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gul Moonis - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Justin Cottrell et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



